kaiser permanente appeal form
KPIC Self-Funded EPO or Self-Funded Product. For more information on the provider appeals processes call.
Kaiser Permanente Ns 1062 2003 2022 Fill And Sign Printable Template Online Us Legal Forms
A member complaint or grievance may relate to quality of care access to services providerstaff attitude or any number of other reasons.
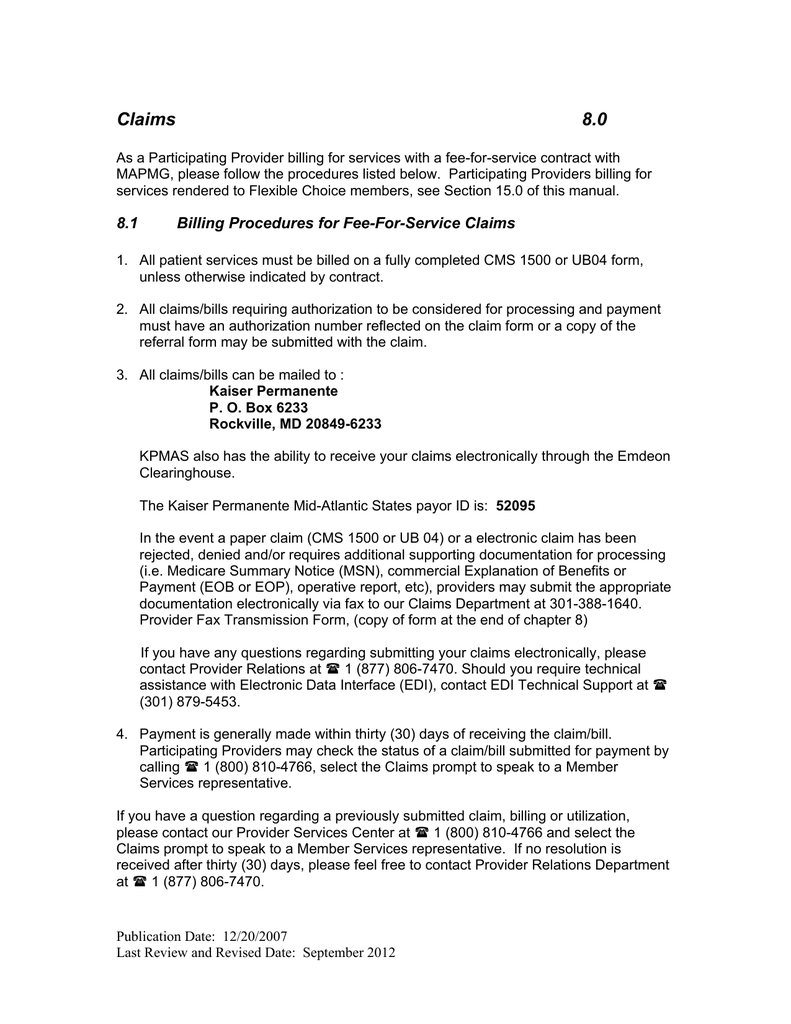
. Original Claim Amount Billed. Please tell us your location so we can take you to information customized for that area. Box 261130 Plano TX 75026.
KPIC Deductible for Individuals Product or Fully Insured EPO. Address Medical Record Number. GrievanceAppeal FORM - Medicare Southern California MemberPatient Name.
Floor Baldwin Park CA 91706. Reason for denial member name medical record number service dates and. Return completed form to.
Complete the Member Appeal Request form PDF and return it to the Member Appeals department using one of the following delivery options. Fillout this form completelyand sign it. Kaiser Permanente Provider Appeals Provider Contracting and Relations 500 NE Multnomah Blvd Ste 100 Portland OR 97232 503-813-3376 503-813-2017 Fax.
Kaiser Permanente Insurance Company INSTRUCTIONS. Either writing to Kaiser Permanente Special Services Unit PO. 1011 Baldwin Park Blvd 1.
For your claim to be considered for payment follow these simple steps. Providers are obligated to make these forms available. We will get back to you shortly.
Please note that all claim payment appeal requests must be filed within 365 days of the date the claim was originally processed or denied in order to be considered for payment by Kaiser Permanente. How to Appeal Mail PO. Denver CO 80237-9998.
Appeal determinations in the brochure begin at the time a claim for benefits or appeal is filed in accordance with these claims procedures without regard to whether we receive all. Patient Date of Birth. Appeal is submitted without Appeal Filing Form the.
Information listed below must be present. Call Member Appeals Toll-Free 1-866-458-5479. If a member wants to file a grievance please have them complete one of these two forms and return it to Kaiser Permanente as instructed on the form.
Please return form to. Street City Zip Code. Box 7136 Pasadena CA 91109 or calling our Member Services department at 1-800-464-.
Oregon SW Washington. Maryland Virginia Washington DC. Kaiser Permanente Member Appeals PO.
An inventory of all forms for health services billing and claims referrrals clinical review mental health provider information and more. Find forms for health services billing and claims referrals and clinical review behavioral health services provider information and more. Kaiser Permanente Claim ID Number.
Kaiser Foundation Health Plan of the Northwest Member Relations Department 500 NE Multnomah St Ste. Then you must send Kaiser Permanente Member Appeals. Provider reconsideration process The claims payment review and reconsideration steps include.
Get an itemized bill from your provider detailing the charges see SectionB for the information. Take advantage of helpful wellness resources learn more about possible health concerns discover in-depth information on drugs and natural medicines and check out our healthy living programs and classesTake advantage of helpful wellness resources learn more about possible health concerns discover in-depth information on drugs and natural medicines and check out. At Kaiser Permanente we welcome the opportunity to share our experiences and ideas with audiences of all types and sizes.
Flexible Choice Options 2 and 3. Original Claim Amount Paid. To help us make the most informed decision about your request for one of our leaders to speak at your event please complete the following questions.
This form is used to request copies of your medical records billing information and other documentation from Kaiser Permanente. If you need a fast appeal due to a life-threatening situation call us. If you have ever wanted to access your medical records from Kaiser Permanente you will need to fill out and submit a Kaiser Records Request Form.
Seattle WA 98124-1593 ATTN. Kaiser Permanente Medical Record Number. Institutional providers may also refer to the applicable institutional provider manual.
Member Care Transition Form. Health Care andor Financial Dependent Power of Attorney form stipulating you are currently authorized to appeal on behalf of the member. Please tell us your location so we can take you to information customized for that area.
Kaiser Permanente Member Services Main Office. Appeal Decision Timelines. You contact our health plan and make your appeal Submit your request for a standard appeal in writing by fax mail or online through the Kaiser Permanente member website see below for contact information.
Member Relations Grievance and Appeal Form Author. Guidelines on submitting requests for radiology services which services require prior authorization and which services do not. Sign in to the secure Kaiser Permanente member website and submit the Online Member Appeal Request.
View download or print commonly used forms guidebooks handbooks and other publications. Other documents and forms. Information on how to submit changes or updates to your provider information so Kaiser Permanente can maintain an accurate provider directory.
Box 34593 Seattle WA 98124-1593. Medicare Advantage Appeals Process Level WrittenVerbal Resolution Maximum timeframe from contact date not including extensions. Preparing for your Appointment with a Non-Kaiser Permanente Provider.
PPO Flyer for Physicians and Care Providers. This form is to request reimbursement for services youve paid for out-of-pocket. If you are the treating provider submitting this request on behalf of a member you must submit an.
CO PPO Member Resource Guide. 100 Portland OR 97232 Fax 1-855-347-7239. KP HAWAII PROVIDER APPEALS CLAIMS ADMIN DEPT PO BOX 378021 DENVER CO 80237-9998.
Choice Products Medical Claim Form.
2
2

Kaiser Provider Appeal Form California Fill Online Printable Fillable Blank Pdffiller
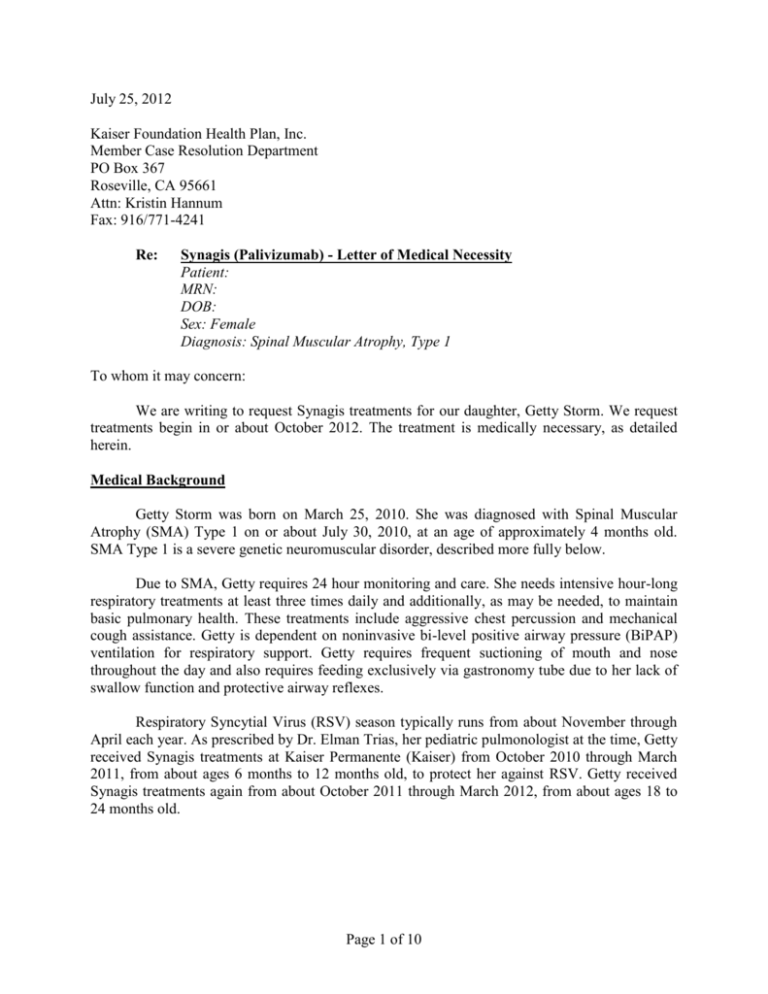
July 21 2012 Getty Owl Foundation
2
Kaiser Permanente Grievance Form Southern California 2020 2022 Fill And Sign Printable Template Online Us Legal Forms
2
2

Kaiser Appeal Form Fill And Sign Printable Template Online Us Legal Forms
Application Kaiser Permanente California
Fillable Online Appeal Request Form Seneca College Residence Fax Email Print Pdffiller
Fillable Online Mydoctor Kaiserpermanente Kaiser Permanente Authorization For Use Or Disclosure Form Fax Email Print Pdffiller
Claims 8 0 Kaiser Permanente
2

Kaiser Permanente Combined Disclosure Form At Your Service
2
Kaiser Provider Appeal Form California Fill Online Printable Fillable Blank Pdffiller
2
Application Kaiser Permanente California